While available pre-operation data such as MRI (Magnetic resonance imaging), X-Ray, or CT (X-ray computed tomography) images can support the surgeon, matching its information to the changed orientation of the patient on the operating table poses a challenge due to the shift of inner organs, the occlusion of the target by interposed tissue, and the degradation of the endoscopic image due to interference inherent to the surgical procedure itself (blood, smoke from electrical cutting and cauterization). A navigation system capable of identifying anatomical markers gained in the pre-operation data during the actual operation and making it available to the surgeon in the endoscopic image would accelerate surgical procedures, limit the tissue damage to the patient, increase the chance of success and improve the recovery of the patient.
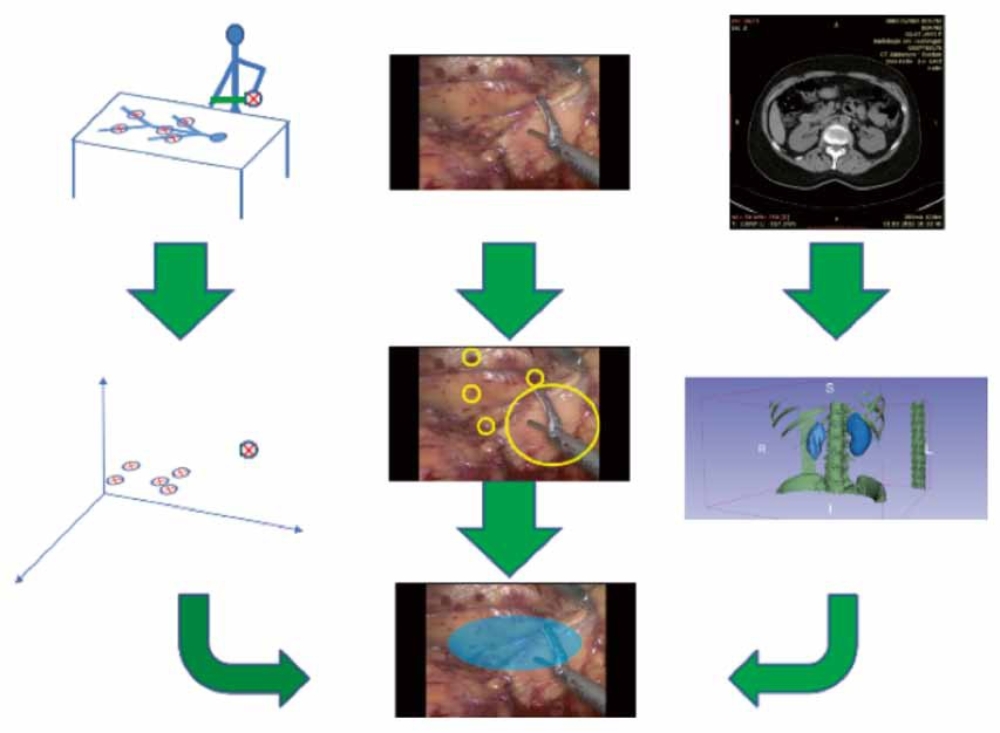
The approach taken in this project involves three stages: 1) the creation of a 3D-model of the patient based on pre-operation CT data, 2) the registration of the absolute position and orientation of the patient and the surgical tools
in the fixed coordinate system of the surgical theatre using optical, inertial, and ultrasonic tracking, and 3) matching the image of the endoscope to the 3D model (fig. 1). The project involves the ISYS (optical, inertial, and ultrasonic tracking) and the ITO (3D Model from CT data) at University of Stuttgart, as well as the Institute for Cognitive Systems (tracking markers in the endoscopic image and blending the CT data into images) and the UKT (medical expertise, test Ops and provision of CT data) at the University of Tübingen.
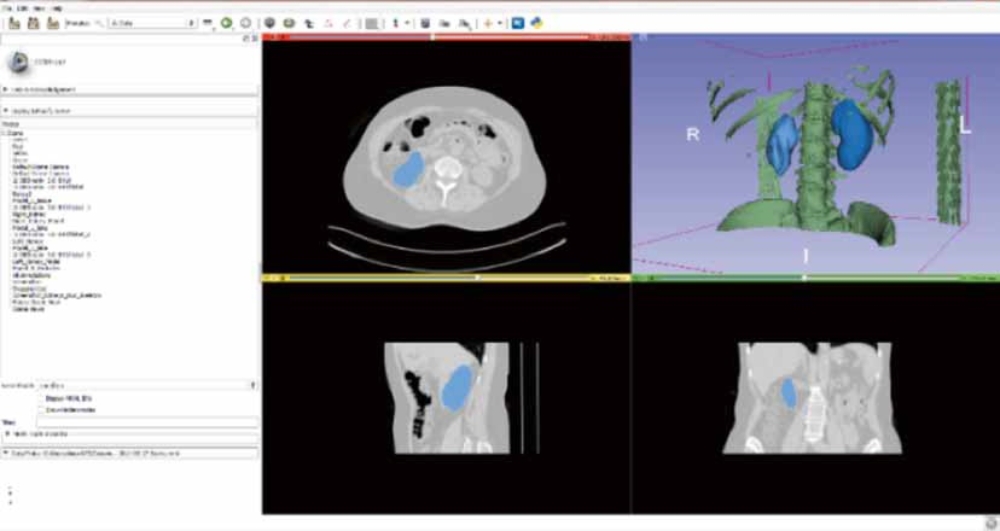
The role of the ITO consisted of the segmentation of CT/MRI data to identify relevant anatomical structures for the creation of a preoperative, patient-internal coordinate system and corresponding 3D model. Since the segmentation and 3D modelling of CT data is a well-researched field with powerful, free and commercial software solutions available, we chose 3D Slicer for this task. In a first step, the skeleton was segmented using a simple thresholding algorithm applied to the Hounsfield coefficients of the CT data set. The skeleton plays key role in the 3D model as it provides easily
identifiable anatomical markers (the pelvic bone or the lower ribs) and a relatively rigid framework. In a second step, the general position of the kidneys was marked manually and the kidneys themselves segmented using a robust statistics segmenter starting with those manually placed seeds. The final 3D model combines these two features and is stored in VTK, PLY, or STL format for further processing (fig. 2).
A test surgery creating one fully consistent data set of CT, registering of the body and the surgical tools in the surgical theatre, and recording the endoscopic image has been performed to test the current state of the the system to be developed in this project.
Supported by: Industry on Campus Project Project: IoC104 – In cooperation with: Aesculap AG, ISYS (University of Stuttgart), Cognitive Systems (University of Tübingen), UKT (University of Tübingen)